After talking to Dr. B, David and I have come up with our game plan. I won’t go into the comfort care procedures we will or will not do, but I will go into how we intend to treat her. A lot depends on how she fares outside of my body.
Here are our odds with a vaginal birth:
7% died in utero
18% died during birth
26% lived between 1 and 60 minutes
27% lived between 1 and 24 hours
17% lived between 1 and 5 days
5% lived 6 or more days
Our odds with a cesarean:
4% died during birth
53% died within 24 hours
30% lived up to 5 days
13% lived longer than 6 days
We know that 9% of these babies die from other defects or a complication from them, another percentage dies from, essentially, heart failure or respiratory problems, and then others from infection. I’ve found no other causes of death so far.
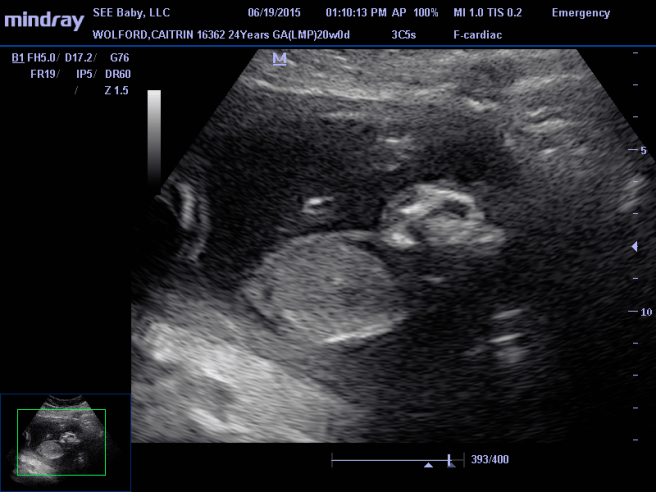
Here’s what we know about Brielle:
She’s strong and all of her organs are healthy and growing as they should. She does not have any other defects. And most importantly her heart is strong. She also has brain matter and theoretically is rewiring her brain to keep herself functional (this is called neuroplasticity).
Here are the ifs:
If Brielle survives delivery and if her lungs form and function correctly, and if we can minimize brain tissue loss from amniotic fluid (hopefully by keeping the fluid clean), and if she stabilizes after she’s born, (meaning her oxygen and blood pressure stay steady) then we can put a plan into action.
So here’s my plan. David and I learn as much as we can about procedures that have been done for anencephaly patients (including the doctors and hospitals involved) and present it to a pediatric neonatologist. We find someone who will help us. We give an allotted amount of time, determined by a doctor, to make sure she is strong and her vitals are steady. We begin antibiotics to prevent infection from her exposed brain and then we implement a procedure to cover the exposed brain and essentially build her a skull. And then, hope for the best.
Here’s the problem, there has only been a handful of these procedures done in the world. Very, very few doctors are willing to change their mindset of anencephaly, let alone, treat it. And we have no idea what to expect if we can treat her.
If you want to help us with our “Save Brielle Mission” you can pray. I don’t care what your faith is, we’ll take all the prayers we can get. And if you really want to get into the nitty gritty, you can help us research people who have helped these babies. We need to have a presentation ready in 11 weeks. As always, you can love our baby girl and cheer for her to make it, just as you all have already been doing. And you can also tell others how special these babies are and how worthy they are of love and life.